Dr. Boehne and Dr. Shane White co-authored Chapter 7: Complications During Restoration of Endodontically Treated Teeth in Dr. Mahmoud Torabinejad’s Management of Endodontics Complications. This chapter highlights common mistakes made in the restoration of endodontically treated teeth, with strategies to avoid them and procedures to correct them.

Effectively cleaning the deepest, most complex portions1,2 of the root canal system requires incredible innovation—and we are proud to offer that technology with the GentleWave® Procedure.
The GentleWave Procedure is a state-of-the-art alternative to standard root canal treatment. The ultracleaning technology of the GentleWave Procedure is an advanced combination of fluid dynamics and a broad range of soundwaves that work together to reach into the microscopic spaces1,2 and remove bacteria, debris and tissue2. The GentleWave Procedure is so effective at cleaning and disinfecting the root canal system, there’s less chance of failure over time.3

The GentleWave Procedure uses a minimally invasive1 protocol to access the infected root canal system, which means it is preserving more of the natural tooth and, in doing so, is helping to keep the tooth’s structure strong. With the GentleWave Procedure we can also typically clean and fill the tooth in just one appointment3, which may reduce the number of appointments required.
Dr. Boehne is honored to have been named one of the Top 40 Under 40 Dentists by Incisal Edge Magazine.
In its fall 2017 edition, Incisal Edge, the leading lifestyle magazine for dental professionals nationwide, celebrates America’s finest young practitioners for their achievements in dentistry.
Incisal Edge celebrates dentists’ achievements both inside the operatory and during their hard-earned downtime — and nothing better exemplifies this than the magazine’s annual 40 Under 40 edition, a series of informative profiles of the finest young practitioners in the dental profession. Whether they’re renowned for their medical innovations, their volunteer work and philanthropy or simply their commitment to outstanding patient care, these 40 honorees— nominated by industry experts from around the country and vetted by an independent panel — represent the best of dentistry today, and the promise of even better dentistry tomorrow.
“The Incisal Edge ‘40 Under 40’ are through the sheer force of their commitment and expertise, helping our profession ascend to even greater heights in the years ahead,” says Chuck Cohen, founder of Incisal Edge dental lifestyle magazine. “We are very proud to honor the brightest rising dental stars in the U.S.”

Dr. Boehne shares the cover of the 2017 fall edition of Incisal Edge with some of the country’s best dentists.
 Dr. Boehne’s latest article Contemporary Endodontics – A Less Invasive Strategy for Long-term Success is out in the August 2017 issue of DentalTown magazine, where he is featured on the cover and featured in a practice profile as well.
Dr. Boehne’s latest article Contemporary Endodontics – A Less Invasive Strategy for Long-term Success is out in the August 2017 issue of DentalTown magazine, where he is featured on the cover and featured in a practice profile as well.
If you don’t have your hard copy you can view the online version here
Dr. Boehne and Dr. Shane White co-authored Chapter 3: Endodontic Complications in the new edition of Best Practices in Dentistry, Avoiding and Treating Dental Complications. This chapter highlights common mistakes made in endodontics, with strategies to avoid them and procedures to correct them. From diagnosis to repair of apical post perforations, this chapter is an exciting read for dental students, endodontic residents, general dentists and endodontists. 
Best Practices in Dentistry is available here:
https://www.amazon.com/Avoiding-Treating-Dental-Complications-Practices/dp/1118988027
Pick up the Spring 2016 edition of Incisal Edge to read Dr. Boehne’s latest article on endodontics. Or preview the article here: Incisal Edge
Pick up a copy of Disinfection of Root Canal Systems: The Treatment of Apical Periodontitis. Dr. Boehne’s cases are used to illustrate how apical negative pressure irrigation can help to effectively clean root canal systems.
Dear UCLA Class of 2017,
Welcome to your Endodontic Technique Course, RFE 209! This should be an exciting quarter, as you will all be completing RCT on each tooth category. A few tutorials are up on this website, under the “dental students” tab. In the past, these tutorials have been beneficial supplements to your lab manual. In addition, I will bring a microscope with co-observation binoculars to facilitate hands-on teaching. Feel free to ask me questions about your cases, and we can go over them together under the scope. Please let me know if you have any requests for specific tutorials, and I will upload them to this website. I look forward to seeing you all next week.
All the best,
Dr. Boehne

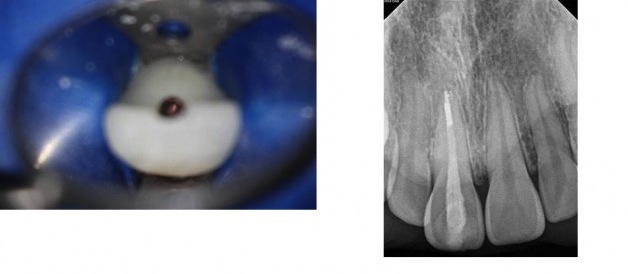
I was asked to post a tutorial with tips on accessing anterior teeth. Please follow the manual for outline form. The purpose of this tutorial is to understand the direction you need to direct your access to locate the canal(s). This is where the most common and detrimental mistakes are made with anterior access. Generally, the shape of the access cavity for an anterior tooth will be an upside down triangle, with the apex of the triangle incisal the cingulum and the base of the triangle somewhere below the incisal edge. It is important not to extend the access below the cingulum, because the cingulum gives the tooth a lot of its strength, so we don’t want to needlessly cut it away. It is nice to not cut the incisal edge, to preserve its integrity and esthetics. As you will see below, sometimes it is necessary to cut the incisal edge in calcified cases. The purpose of making it a triangle is to clean out the pulp horns. You will notice in the case below that my access is not a triangle, this is simply because it was a very calcified tooth with no pulp horns. You guys will be treating teeth with wide open pulp chambers and pulp horns, so for the class and boards, the outline of the access cavities should look like they do in the manual.
Accessing anterior teeth is very difficult because it is difficult to appreciate the direction of the long axis of the root when we are initiating the access from the lingual side of the crown. These teeth are skinny at the neck, so there isn’t a lot of room for error.
There are two very common errors made: (both have to do with improper orientation during access).
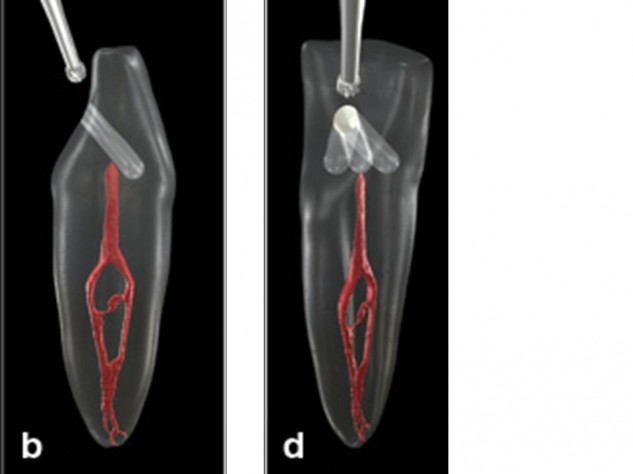
1. Perforating out of the facial side around the CEJ. (pic B)
2. Perforating or gouging mesially or distally. (pic D) Even if you don’t perforate, gouging (drilling away too much tooth structure while looking for a canal) can weaken a tooth enough that the crown can break off.
Notice from the picture above (borrowed from Dentistry Today), that the best straight line access to these teeth would be right through the incisal edge. The reason we access through the lingual side of the tooth is to avoid violating the incisal edge, not because it gives us the best straight line access. In cases where the pulp chamber has not receded, such as the cases you will be treating, you will not need such a vertical angle to find the pulp chamber, and will not need to violate the incisal edge. So, don’t extend your access past the incisal edge. The further your pulp chamber has receded, the more you will have to tip your bur vertically toward the incisal edge to be able to drill down and find it.
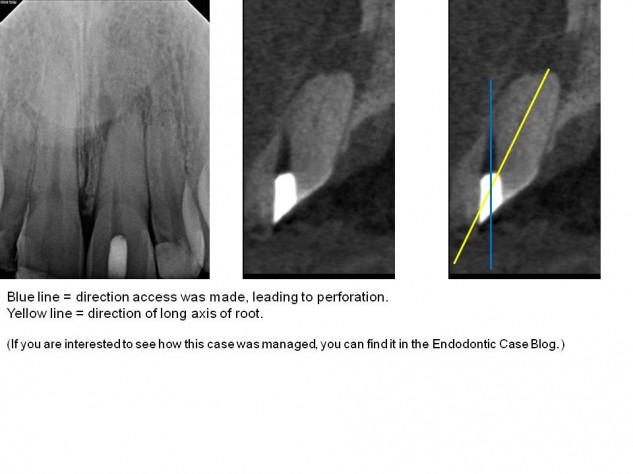
Notice how if we start on the lingual with our bur pointed toward the facial, and continue in this direction, it will lead to a perforation out of the facial side of the tooth. The sagittal CBCT image below is an example of a case where a dentist did just that. Notice how the canal is located in a completely different direction from where they were looking. This common error is due to accessing from the lingual, but not realizing you still need to be oriented down the root.
This is an extreme example to illustrate the point of long axis. This was a very calcified case. CBCT showed that I wouldn’t expect to find a patent canal until 16.5mm. Note that if access was oriented from the lingual in a buccal direction, drilling 16.5mm would not only perforate the facial side of the tooth, but possibly the patient’s lip.
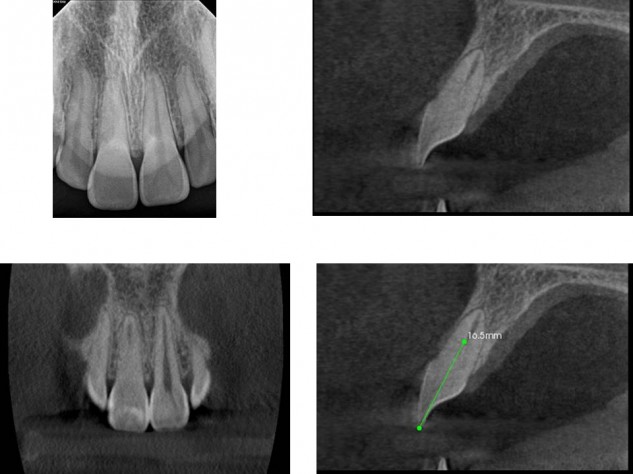
This case was so calcified that I took an interoperative CBCT to make sure I was in the long axis of the tooth in three dimensions. If you are getting nervous drilling down into the root, it is always good to stop and get images to see where you are.
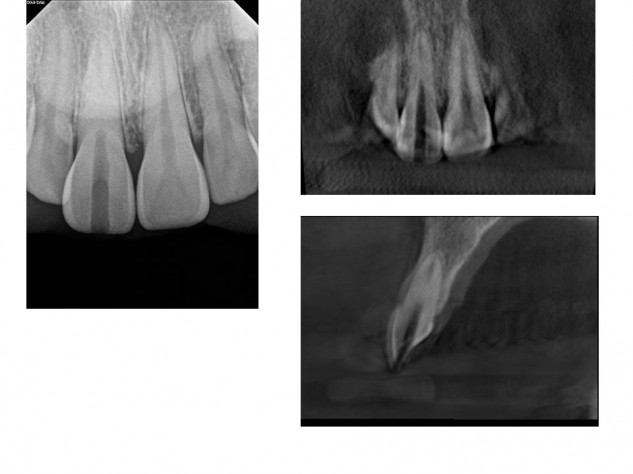
By remaining in the long axis of the root, the canal was eventually located without procedural errors and treatment was completed.
The take – home points are:
1. Use the triangular outline form shown in your manual, because you will have pulp horns.
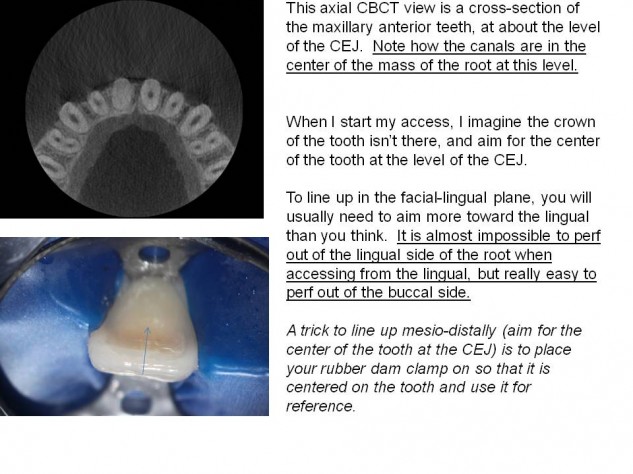
2. Understand where the long axis of your root is, in relation to the cavosurface margin of your access cavity. When accessing from the lingual, aim more lingually than you think (drill in the direction of the root, not perpendicular to the lingual surface of the tooth). Avoid weakening teeth with mesio-distal gouging.
I recommend taking photos of your teeth from the side before you mount them. I also recommend having another unmounted anterior tooth out to reference. If you are accessing and don’t find a canal at the level you think you should, stop and take a radiograph.